- Visibility 141 Views
- Downloads 32 Downloads
- Permissions
- DOI 10.18231/j.ijca.2019.121
-
CrossMark

Abstract
Central venous catheter (CVC) placement is indicated for various therapeutic and diagnostic purposes. However, it is important to ensure its proper placement. A CVC malposition is associated with number of recognized complications, some of which can be fatal.
Case: In a 27 year female admitted in ICU with history of seizures and oral bleed with stable vitals, 7Fch subclavian CVC was inserted. She had progressive dyspnea, chest pain and hypotension. Although chest X-ray showed correctly positioned CVC, CECT chest showed it was entering SVC, traversing along its medial wall and reaching between SVC and aorta and entering in the right atrium. Also atelectic fluid in oblique fissure, bilateral pleural effusion and small pocket of air in anterior mediastinum with minimal mediastinal high attenuation collection was seen. This was removed and patient was under observation for 24 hours, after which she was shifted to ward.
Conclusion: Therefore location of the catheter must be verified by radiological methods. Also real-time ultrasound reduces the number of complications associated with the technique.
Introduction
Central venous catheter (CVC) insertion is indicated for various therapeutic as well as diagnostic purposes in patients admitted in intensive care units (ICU), various dialysis units and in routine and emergency operation theaters. However, it is important to be sure of its proper placement. A CVC malposition can be associated with large number of recognized complications, some of which may be fatal. These may occur either during insertion of the catheter (e.g. arterial puncture, pneumothorax, arrhythmias), and/or during maintenance of the line (e.g. infection, thrombosis). Variousmal positions of CVC can be its placement in internal mammary vein, coiling within the vein itself, migration of catheter to ipsilateral jugular vein from subclavian vein or translocation to the contralateral subclavian vein etc.[1],[2],[3] Pericardial effusion and pericardial tamponade are rare but accounting for up to 0.7% of central venous catheter related complications[4],[5] Recommended use of post-insertion chest radiograph or using any other radiological method for the confirmation of correct placement and detection of complications like pneumothorax should be employed.
Here we present a very rare case of mal positioned central venous catheter vein entering into superior part of superior venacava (SVC), traversing along its medial wall and its tip reaching up to the junction between SVC and aorta. However, the terminal end was in right atrium.
Case presentation
A 27 year old woman on her post-partum day 27 was admitted in emergency room following 5 grand mal seizures within a period of 6 hours. Due to the seizures she had tongue and lip bite followed by bleeding and edema. For the control of fits she was shifted to ICU. On examination she was slightly drowsy. The pulse rate was 9 0 per minute and blood pressure was 13 0/80 mm Hg. MRI brain was within normal limits. Injection Clonazepam was given intramuscularly and phenytoin bolus followed by thrice a day dose was given. She was oxygenated using high flow oxygen mask and X-ray chest was done ([Figure 1] - some hilaropacity in otherwise normal lung). As there was no peripheral venous access due to previous injuries and cut downs, a 7 Fchpolyvinyl chloride subclavian line insertion was planned using landmark technique in the right infra clavicular area to facilitate the administration of intravenous drugs and fluids. A free flow of blood back down the catheter was noted after insertion.
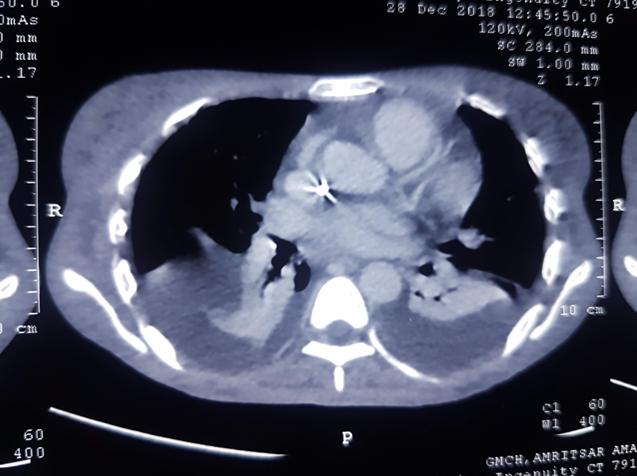
Eventually, her seizures settled and on day 4 she was shifted to ward with stable vitals. Two days later we received her back in ICU with the compliant of severe dyspnea and precordial pain overnight. Another chest x-ray ([Figure 2] - showing basal homogenous opacities suggestive of aspiration pneumonitis with bilateral blunt CP angles suggesting mild pleural effusion. The central line was below carina so it was slightly readjusted). As she was diagnosed with aspiration pneumonitis and the treatment was started for the same. But her dyspnea persisted and was later accompanied with hemodynamic instability (day 8). At this time, despite increased volume administration, increased norepinephrine dosing was required to maintain an adequate mean arterial pressure. A contrast enhanced CT chest was planned and it showed massive bilateral pleural effusion (more on right) especially on dependent parts with atelectic right middle lobe and consolidation present. Also fluid was seen in oblique fissure of lung. Mild pericardial high attenuation collection with mediastinal collection effusion with cardiomegaly was present. The CVC was seen in right subclavian vein entering into superior part of SVC ([Figure 3]), traversing along its medial wall and its tip reaching up to the junction between SVC and aorta ([Figure 4]). The terminal end appeared to be in right atrium. Small pocket of air was also noted in anterior mediastinum with minimal mediastinal high attenuation collection. The air in mediastinum was due to the small air instilled during the transfusion of fluids.
A peripheral line was secured and this mal positioned catheter was removed and patient was kept under observation. Patient was hemodynamically stable for 24 hours after which she was shifted to ward.




Discussion
Since the introduction of CVC insertion in 1945, this has been widely used. More than 15% of patients undergoing CVC placement presented with complications out of which 5% to 19% were mechanical, 5% to 26% were infectious and 2% to 26% were thrombotic in nature.[6]
In the year 1979, Duntley et al. studied 34 case reports and observed catheter-related vessel injury and resulting hydrothorax in 61 patients.[7]
It was thus considered that majority of known vascular complication during insertion of central line is due to the mishandling and inexperienced manipulation of the dilators. Second possible mechanisms that may be thought of include kinking of the guide wire while insertion, hence causing misdirection of the advancing dilator. Thirdly, it can also be due to insertion of the guide wire outside the vessel.[8] All these complications are generally due to inexperience, increasing the number of attempts, using a larger gauge needle, morbid ly obese patient and in patients with underlying coagulopathy.
Cases have been reported in the past that showed development of hydro-mediastinum and bilateral hydrothorax after a subclavian line insertion.[9] These patients were diagnosed when they complained of tachypnea, tachycardia and hypotension after placement of CVC. The authors stated that probable mechanism of injury of vein during the process of cannulation was the dilator mishandling and resulted in hydro-mediastinum, as occurred in our case and shift of fluid from the mediastinum into the pleural cavities causing bilateral hydrothorax.
A similar and rare case of a central venous catheter (CVC) inserted through the left internal jugular vein that perforated the superior vena cava (SVC) wall was also reported by Kurabe M et al.[10]
In our case diagnostic CT scan done for chest pathology incidentally showed mal positioned central line. This could be the probable cause of increasingly worrisome symptoms of tachypnea and precordial pain, both of which improved gradually after CVC removal. In such kind of scenario, it is recommended to stop all the running infusions through the CVC followed by its removal under specialist supervision. If still symptoms persists, a trained person should perform pericardio-centesis..
Conclusion
Subclavian catheter insertion in practice may cause serious complications which can lead to death. Therefore, the procedure of CVC insertion should be performed by trained and experienced hands or under real time radiological guidance such as ultrasonography. Since blood aspiration from the catheter is not reliable indicator to exclude vascular perforation, I conclude that the locat ion of the catheter must be rechecked by radiological methods. Also real-time ultrasound reduces the number of complications associated with the technique.
Competing interests
None.
References
- Kela M, Munde H, Raut S. Accidental placement of central venous catheter into internal mammary vein: A rare catheter malposition. Ann Card Anaesth. 2017;20:477-485. [Google Scholar]
- Tomar GS, Tiwari AK, Jain DG, Chawla S, Sinha R. Central venous catheter rotation malposition: An unusual presentation. Indian J Anaesth. 2012;56(4):415-415. [Google Scholar]
- Bansal S, Bansal S, Dogra M, Khan I. A malpositioned central venous catheter. Pain Intensive Care. 2019;26:54-56. [Google Scholar]
- Nowlen TT, Rosenthal GL, Johnson GL, Tom DJ, Vargo TA. Pericardial effusion and tamponade in infants with central catheters. Pediatr. 2002;110(1):137-142. [Google Scholar]
- ECW, Pelausa EO, Allen AC, Stinson DA, Hanna BD. Massive pericardial effusion as a cause for sudden deterioration of a very low birthweight infant. Am J Perinatol. 1993;10(6):419-423. [Google Scholar]
- Merrer J, B DJ, Golliot F, Lefrant JY, Raffy B, Barre E. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. JAMA. 2001;286:700-707. [Google Scholar]
- Duntley P, Siever J, Korwes ML, Harpel K, Heffner JE. Vascular erosion by central venous catheters. Clinical features and outcome. Chest. 1992;101:1633-1638. [Google Scholar]
- Hohlrieder M, Oberhammer R, Lorenz IH, Margreiter J, Khbacher G, Keller C. Life-threatening mediastinal hematoma caused by extravascular infusion through a triple-lumen central venous catheter. Anesth Analg. 2004;99:31-35. [Google Scholar]
- Naguib M, Farag H, Joshi RN. Bilateral hydrothorax and hydromediastinum after a subclavian line insertion. Can Anaesth Soc J. 1985;32:412-414. [Google Scholar]
- Kurabe M, Watanabe T, Kohno T. Perforation of the superior vena cava 5 days after insertion of a central venous catheter through the left internal jugular vein. J Clin Anesth. 2016;31:193-196. [Google Scholar]