To the Editor,
Central venous catheterization through internal jugular vein (IJV) is routinely done in patients undergoing cardiac surgery. Central venous catheter (CVC) placement may lead to mechanical problems like misdirection, coiling, knotting or looping that causes obstruction or suboptimal functioning.1 We present a case of misplaced CVC tip in a patient who underwent cardiac surgery.
A 45-year average-built male posted for ostium primum atrial septal defect (ASD) closure. His preoperative clinical examination and blood investigations were within normal limits. Transthoracic echocardiography (TTE) showed ostium primum ASD 27mm with left to right shunt with normal biventricular function. The right atrium and ventricle were dilated owing to long standing shunt.
After informed consent standard protocol was used for induction of general anaesthesia (GA) and monitoring. After induction of GA right IJV was catheterized with Seldinger’s technique using CVC (16,18,18G, 7 Fr, 20 cm, triple lumen) Landmark technique with central approach was used to catheterize the IJV. The procedure was uneventful and all lumens were checked for patency. The catheter was secured with suture at the hub.
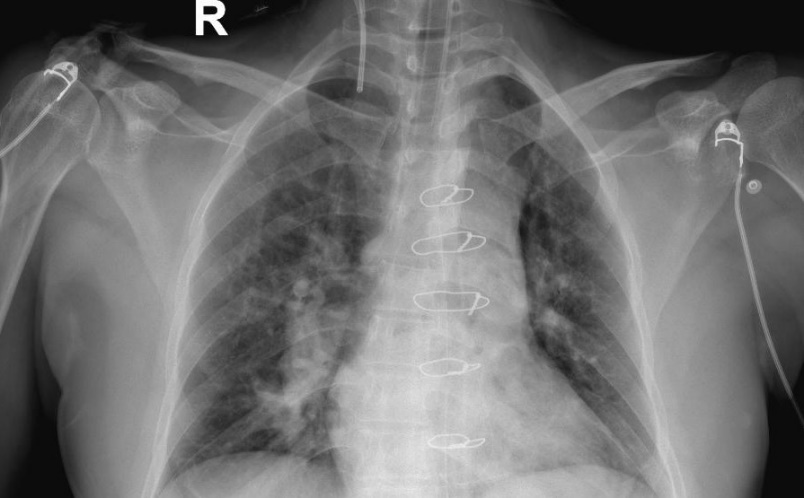
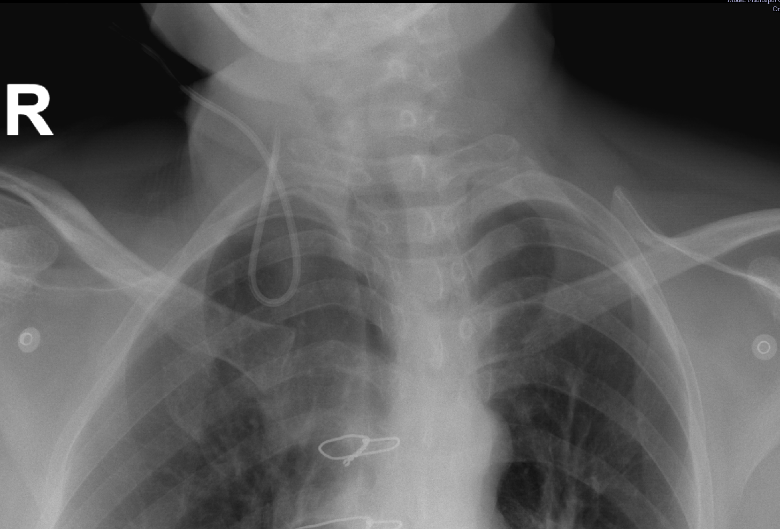
The surgical procedure was uneventful and the patient was shifted to the intensive care unit (ICU) for monitoring and mechanical ventilation. Chest radiograph in ICU revealed higher placement of the CVC and tapering tip of the catheter was also not seen. (Figure 1) On zooming the image all three lumens of the catheter were visualized which look like transection of CVC. (Figure 2) The surgical team also denied accidental cutting the tip of catheter and revealed that the tip of catheter was not visualized intraoperatively. To look for the missed portion of CVC it was decided to repeat chest radiograph including the cervical region which showed looping of the CVC (U-shaped) within IJV. (Figure 3) Rest of the postoperative course was uneventful and CVC was used for infusions and was removed on second postoperative day with intact tip as per our protocol.
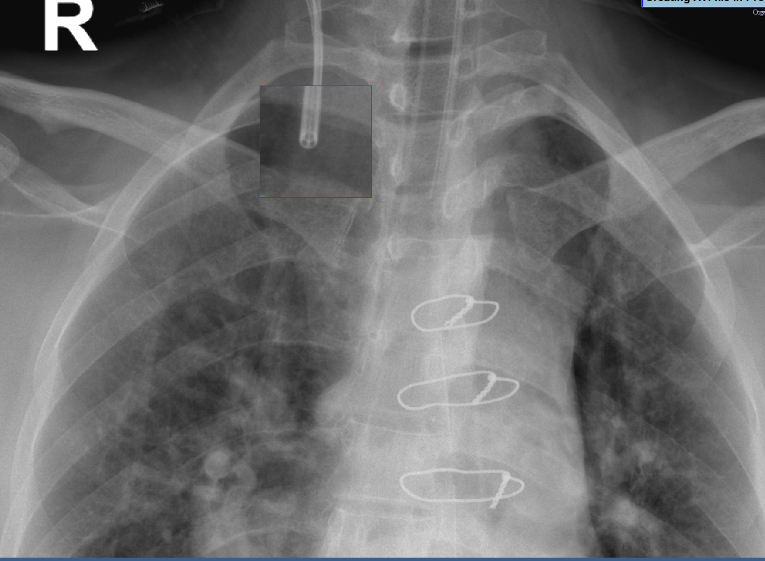
CVC placement may lead to mechanical complications with incidence varies from 6-10% and coiling/looping of the catheter mostly reported with longer catheters like pulmonary artery catheter.2 One of the causes of looping is extra insertion of guidewire or catheter in the vein however that was not the case in this patient. Otherwise, manipulation during superior venacava cannulation may cause dislodgement of the tip of catheter which was again not in this case. In this patient the zoomed radiograph image revealed all lumens of the CVC that lead to doubt of transection of the catheter which is sometimes electively done by surgeons in case of extra length in the surgical field. However, that was also ruled out by the surgical team. Another theory is that venotomy and cannulation of SVC for CPB might lead to displacement of CVC which was again not there in this case.3
Intra-atrial ECG monitoring can be used for positioning of the guidewire.4 In view of above radiograph of abdomen was also done but that was inconclusive and repeat scanning of the chest showed looping of the catheter.
To conclude, looping or coiling of CVC may occur in some patients and radiograph sometimes may lead to misdiagnosis. Therefore, whenever in doubt, repeat radiograph should be done to confirm the findings.